Viral serologies can be really confusing. But, these make really good boards questions for those of us in acute care medicine. In this Twitter post, @POCUSmedicine shares a really nice infographic about Hepatitis B serologies. While the top left corner is specific to HBV, the general pattern of interpreting serology results is true of all viral serologies. I learned a mnemonic to help remember this when I was studying for boards…IgM = iMMediate, as in active infection is present; IgG = Gone, as in previous exposure.
Category: Heme/ID
Calcium in MTP
Transfusing a lot of blood presents a lot of problems (not the least of which being that the patient needs a lot of blood to begin with!). Chief among those is likely the coagulopathy that results from a depletion of coagulation factors due to losing whole blood (PRBCs, plasma, and platelets) but only getting PRBCs back. Massive transfusion protocols (MTP) helps to address this by transfusing additional products in some sort of “proper” ratio (what that ratio IS is up for debate), but even if you transfuse PRBCs, FFP, and platelets in proper balance, you can still run into another life threatening complication. And I’m not talking about TACO (although that certainly is a problem). It’s one that may not be as readily recognized or remembered, but one that can wreak havoc with your resuscitation. Hypocalcemia.
Banked blood contains citrate as a preservative for storage. Citrate binds calcium and renders it inactive. Giving lots of banked blood can result in hypocalcemia. Hypocalcemia can cause all sorts of problems including hypotension (probably ALREADY a problem in someone requiring MTP) and seizures.
Pharmbythegram has a really nice post summarizing the role of calcium administration during MTP. Hopefully, you’ll now always remember to give calcium along with PRBCs, FFP, and platelets.
The Pesky Details of Blood Cultures
When I was a bedside nurse – and even before that, when I was a tech in the Emergency Department responsible for drawing blood – the issue of not being able to get two sets of blood cultures, or not getting enough blood in each bottle, would come up. Some patients are very hard to get blood from and blood cultures are a particularly onerous task. We require two separate sticks (often not drawing these from indwelling lines but requiring fresh sticks) and we require a very specific amount of blood in each bottle. This makes getting blood cultures difficult to obtain.
So, why do we need 2 bottles with 10mls each? As usual, Eddy Joe Gutierrez has the answers. He recently released an episode of his Saving Lives podcast where he discusses this. If you prefer to read, he had a blog post back in October of 2020 that covers the same material. As always, he provides links to the studies so you can check his facts. And let’s all be glad that we don’t routinely require three sets.
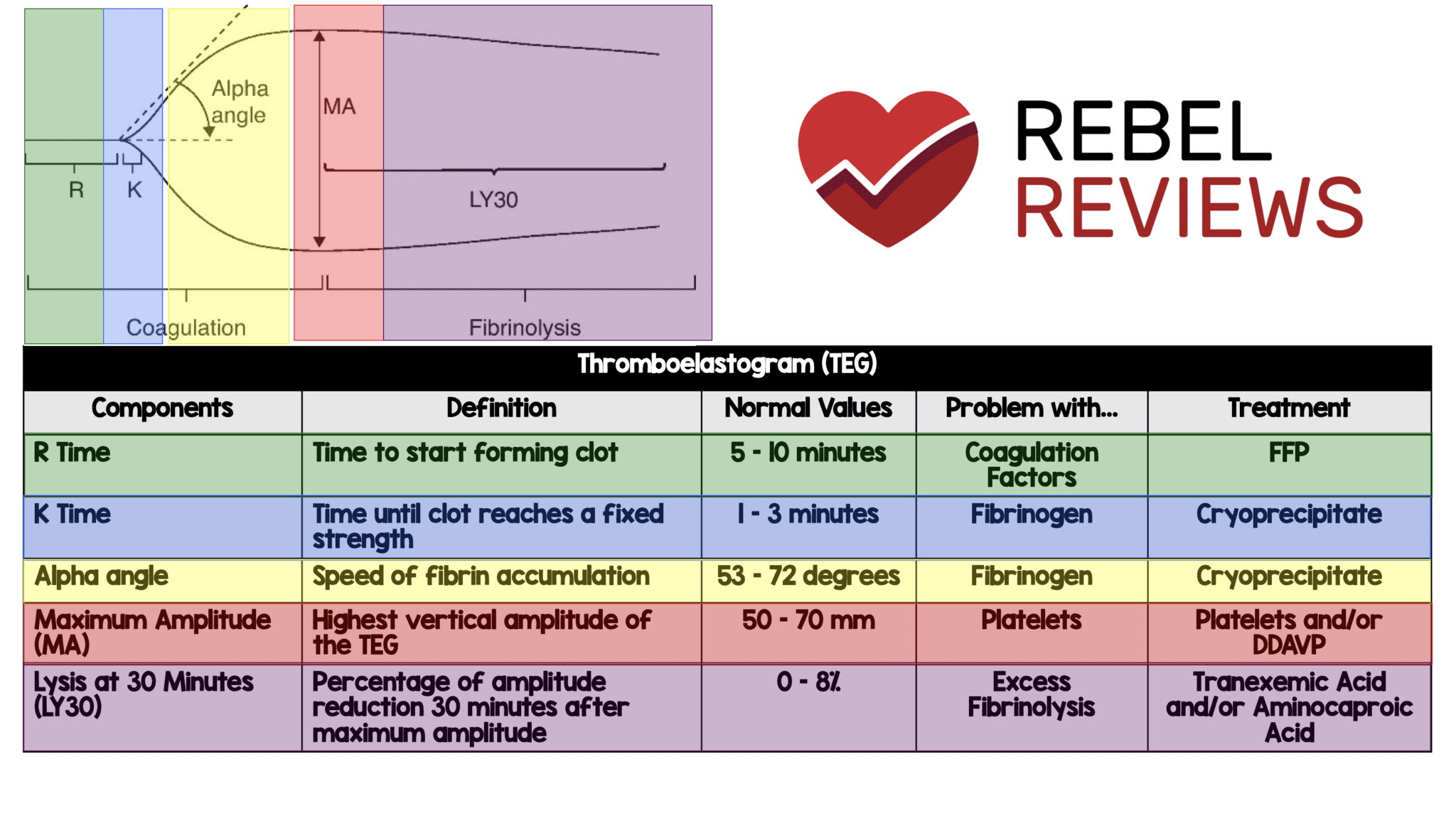
Thromboelastogram (TEG)
If you’re a visual learner like me, you’ll appreciate this TEG quick reference from REBEL EM. It not only covers what you need to know about reading a TEG, but what to do about the abnormal results.