
Have you heard of hepatorenal syndrome (HRS) but don’t really understand it? At it’s core, HRS is renal dysfunction as a result of liver disease. It’s common in patients with end-stage liver disease (ESLD) and among patients undergoing liver transplant. The good news for the kidney is, its not really a kidney problem. It’s a liver problem. So, fixing the liver is the fix for the kidneys. DocSchmidt has a really good Instragram post covering the pathophysiology, diagnosis, and treatment of HRS. All in < 2 mins!
Category: GI/Endocrine
Docusate for Constipation?
A while back, I read an article in a great series from the Journal of Hospital Medicine called, “Things We Do For No Reason” (and they have a Twitter account too!) It’s a great series and there are a lot of articles applicable to the ICU. The series examines things that we in healthcare do, but for which there is actually no good evidence for. The article in question was on the use of docusate for the prevention or treatment of constipation.
This is a drug that used to be on my standard ICU order set. Everyone got it on admission to prevent constipation. But, it turns out that it doesn’t really work. In fact, it’s no better than placebo. So, I stopped ordering it. I took it out of my order set. I use other drugs (like senna and polyethylene glycol) to prevent and treat constipation.
And so I was really glad to see this Instagram post from Doc Schmidt, an actual gastroenterologist also supporting the practice of ditching docusate! Check out his post and read the paper for yourself. Then delete that from your order set.
Liver Function Tests
When I first started in critical care, I got all the various liver function tests (LFTs) confused. Jonathan Downham over at the Critical Care Practitioner, made this great infographic that helps explain which tests tell you what.

And, if you want to go a little more in depth on liver failure, we did a great episode of the Critical Care Scenarios podcast with Elliot Tapper. Dr Tapper goes over everything you wanted to know about liver failure (including why he doesn’t want you to call these tests “liver function tests”).
When to Scope in GI Bleeds
I ran across a great video on Instagram yesterday by one of my favorite GI docs, @docschmidtig. If you’re not already following him, you should, his videos are great! This particular one was funny, but also dealt with an interesting point, why do GI docs wait so long to scope someone with a GI bleed? I liked the video on my IG account, but this morning thought it merited a quick post of its own.
This is something I sometimes get frustrated by (or did until Elliot Tapper set me straight). I’ve got a patient with an obvious GI bleed. I call GI, expecting them to scope and fix the problem. And then it feels like they drag their feet over it. In this video clip, Schmidt explains why.
If you want to delve more into the management of GI bleeding. The aforementioned, always informative Elliot Tapper did an episode of our Critical Care Scenarios podcast not long ago on the subject. Listen here.
PS: If you’re a fan of the TV show M*A*S*H, in episode 4 of season 1, Chief Surgeon Who?, Hawkeye explains a similar rationale to Frank regarding why he’s waiting to operate on the patient in obvious shock.
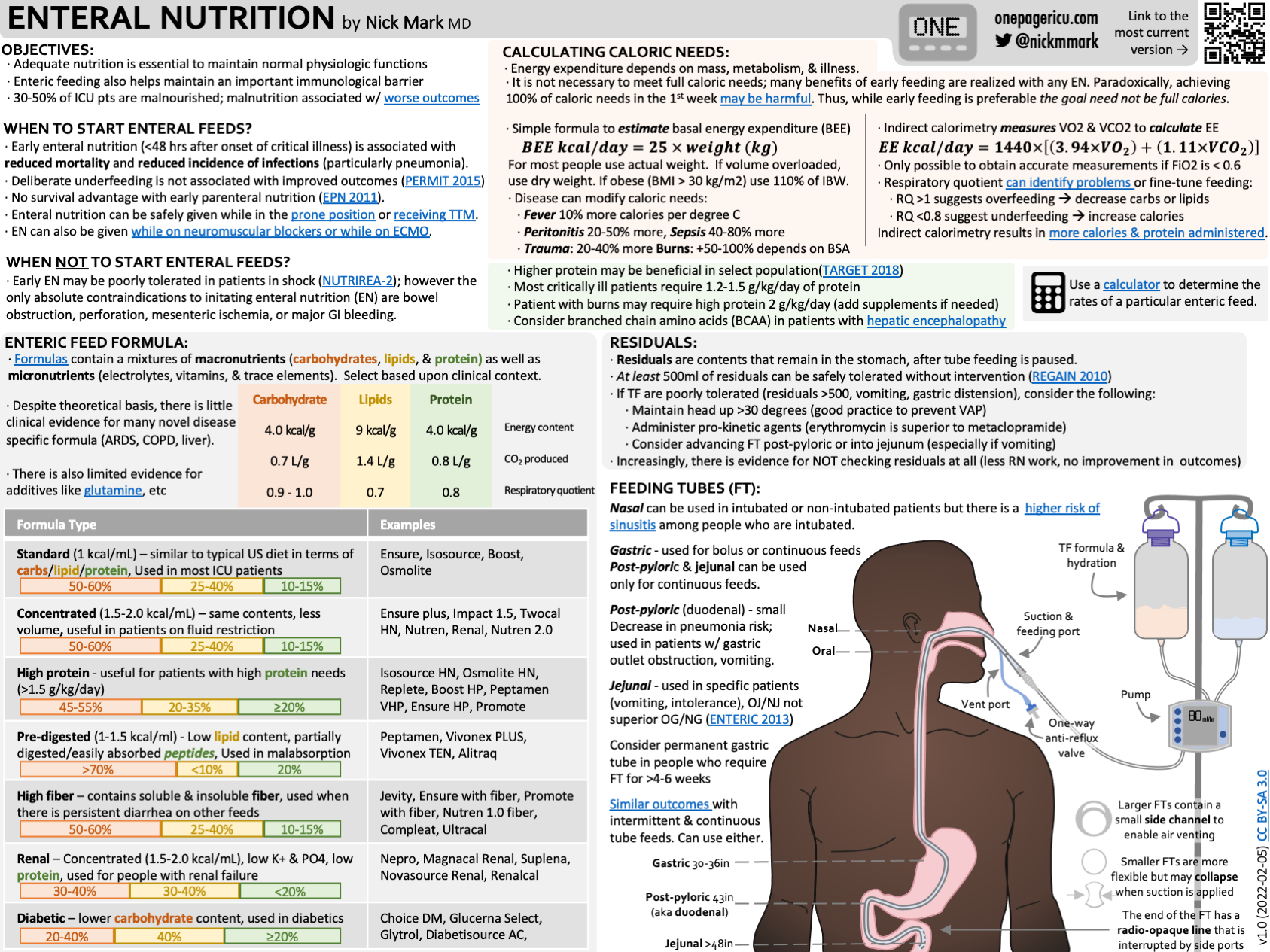
Enteral Nutrition
In medicine generally, and critical care specifically, we’re not always so great about nutrition. After all, that’s why we have dietitians, right? Well, I’ll be the first to say that Registered Dieticians (RD) are invaluable members of the ICU team, and I rely on their expertise daily. However, they’re not always available. Additionally, as ICU providers, we should all be at least somewhat familiar with the basics of nutrition. So, when should we start enteral nutrition? When should we not? OK, we’re going to start tube feeding, which formula? How much?
As usual, Nick Mark over at onepagericu.com has you covered. This great ICU One Pager (PDF or PPT) on Enteral Nutrition covers everything you, as an ICU provider, need to know. This will at least help you get started until you can consult your local RD, or help you to provide proper nutritional therapy for your patients if you don’t have an RD available.
IV Bicarb: Is There Any Value?
IV Bicarbonate used to be all the rage in critical care. It was included in the ACLS algorithms. It was used, in drips or in pushes, to treat all kinds of problems. I’ll admit, there are still times that I use it when the indication is…shaky, often when my back is against the wall and I need something to buy some time. But, is there any real use for it in ICU practice? In a recent episode of The Elective Rotation, Pharmacy Joe recently took a look at when IV bicarb should be avoided (often) and when it is helpful (a lot less often).
Often, IV bicarb is used as a band-aid. This is ok to a point. If it helps buy you some time, ok. But using it without addressing the underlying issues (like I remember doing a lot in the old days) is fraught with problems. There are a handful of scenarios where we should avoid using bicarb because it’s been shown to be of no value. ACLS has removed it from the algorithms and generally avoids against its use in cardiac arrest, for example. But there are some specific times when it is helpful and should be considered.
CT Abdomen and Pelvis Anatomy
I love a good visual guide to anatomy. As someone who looks at more than a few CTs of the belly, this is super helpful in making sense of what I’m seeing. Also, as someone who does a fair amount of POCUS exams of the abdomen, it’s also super helpful.
GI Bleeding
GI bleeding is a common occurrence in the ICU, but do you know how best to handle it? BID PPI or drip? When do you need to call GI for a scope? What about octreotide? In this episode of the Critical Care Scenarios podcast, Brandon Oto and I talk with fan favorite Elliot Tapper about how to approach these patients in terms of diagnosis and management. Lots of great stuff in this one! Listen here.
