
One of the most common procedures that we do in the ICU is place some sort of invasive line in a blood vessel. These may be arterial lines or vascular access lines in the form of central venous catheters or PICC lines. In this episode of the Critical Care Scenarios podcast, Brandon Oto and I discuss how, when, and why we place lines. Listen here.
Author: Bryan Boling
I'm a critical care nurse practitioner and co-director of the Critical Care APP Fellowship Program at the University of Kentucky. I split my clinical time between the Neurocritical Care Service, the Surgical Critical Care Service, and the ECMO Service. I'm also an Adjunct Faculty Member in the Acute Care Nurse Practitioner Program at Georgetown University. I have a passion for education and #FOAM.
GI Bleeding
GI bleeding is a common occurrence in the ICU, but do you know how best to handle it? BID PPI or drip? When do you need to call GI for a scope? What about octreotide? In this episode of the Critical Care Scenarios podcast, Brandon Oto and I talk with fan favorite Elliot Tapper about how to approach these patients in terms of diagnosis and management. Lots of great stuff in this one! Listen here.
Push Dose Pressors
You’re intubating a patient who is hemodynamically tenuous, or worse, was hemodynamically stable prior to induction. After administration of the sedative they become hypotensive. In many cases, the hypotension doesn’t present immediately because of the sympathetic stimulation of the laryngoscope. But once the tube is in and things settle down, the BP starts to drop. What do you do? This is almost always a transient problem. Do you need to start a drip? Anesthesiologists and an increasing number of EM providers use something called “push dose pressors.” Little boluses of vasopressor agents that can bolster your patient’s blood pressure to get them through a transient drop. In this article on Critical Care Now, Ruben Santiago covers the Pearls and Pitfalls with Push Dose Pressors. Although he approaches this from a ED perspective, the concepts are the same for transient hypotension associated with sedation in the ICU.
Propofol and Hypotension
Propofol is a super common medication that we use for induction prior to intubation and for maintenance of sedation in the ICU. One of the big downsides of its use is the risk of hypotension. In this episode of the Elective Rotation podcast, Pharmacy Joe addresses the question “Can hypotension from propofol be predicted?” Although we can and do often use push-dose pressors to deal with this temporary hypotension from propofol and other similar agents in RSI scenarios, there are other situations where adequate sedation with propofol can lead to hypotension. In these situations, are the only answers to switch sedatives, tolerate inadequate sedation, or start vasopressor infusions? Nope. Give this episode a listen to discover more about predicting who will become hypotensive and how to prevent it (in some cases). Listen here.
Are Diuretics Safe in Critically Ill Patients?
One of the more important (and overlooked) aspects of critical care is the concept of de-resuscitation. We give lots of fluid to patients in the throws of shock of all kinds, but even though that fluid resuscitation may be life saving at the time, it can lead to lots of complications later on. So, we need to de-resuscitate these patients and often the best way to do that is with diuresis. But, are diuretics safe to give in the critically ill? In this episode of the Elective Rotation podcast, Pharmacy Joe discusses the safety and efficacy of diuresis in the ICU. Listen here.
CXR Anatomy
One of the hardest things about learning to read any radiology study is understanding the anatomy that you’re looking at. The Radiologist on Instagram posts lots of great annotated images and this one of CXR anatomy is one of my favorites.
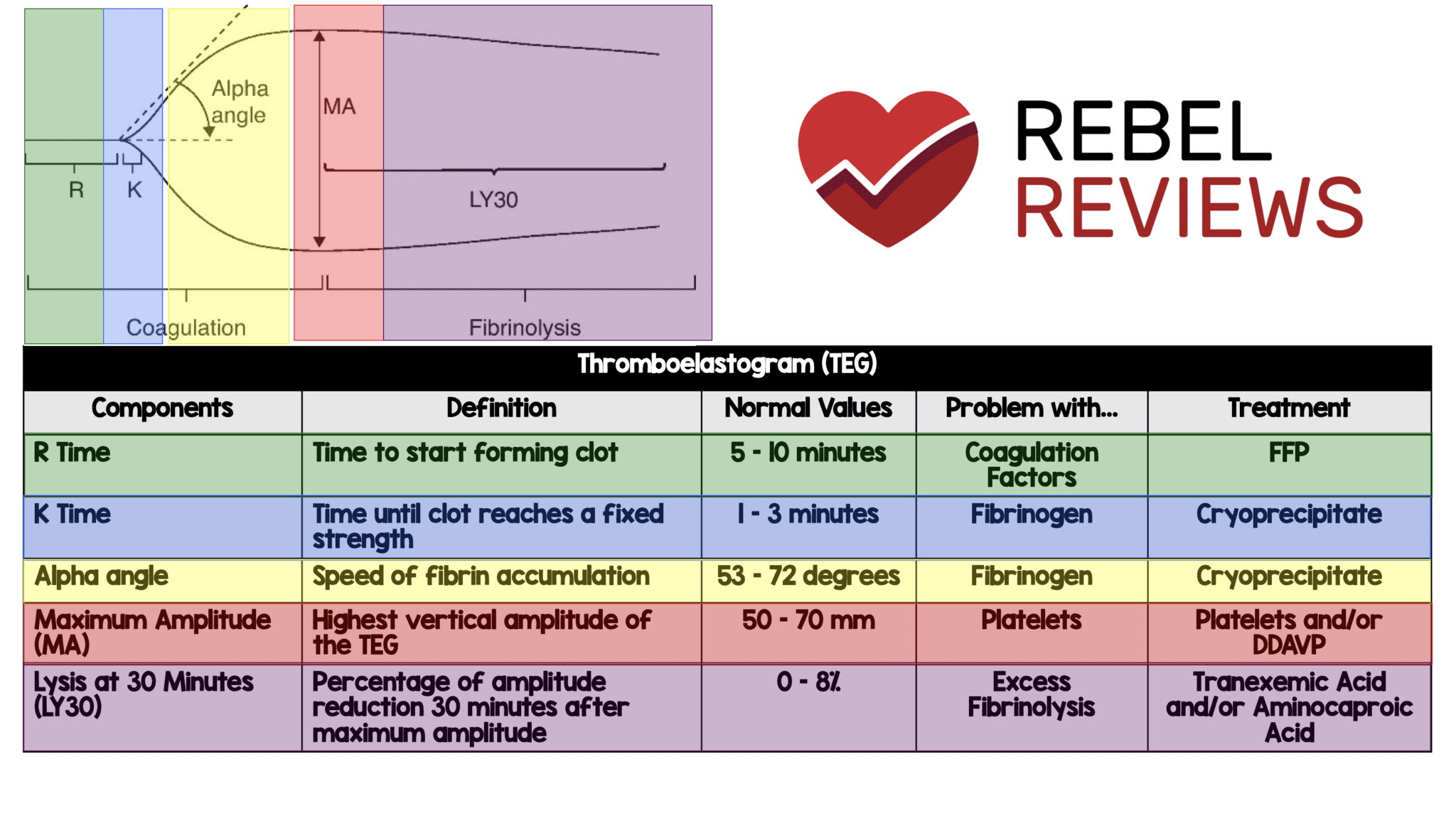
Thromboelastogram (TEG)
If you’re a visual learner like me, you’ll appreciate this TEG quick reference from REBEL EM. It not only covers what you need to know about reading a TEG, but what to do about the abnormal results.
Neurocritical Care Intubation
This is an older episode from the EM:Crit podcast, but it’s good and still mostly true. Part of Scott Weingart’s “The Laryngoscope as Murder Weapon ” series, “The Neurocritical Care Intubation.” This discusses some of the pitfalls in intubating a patient in the neuro ICU and ways to avoid them. Note, we don’t always do these things, but there’s a lot of good stuff in here to talk about.

The Elective Rotation
I found a new podcast this week that I really like, it’s called The Elective Rotation and it’s really for pharmacists, but it’s good really good info for providers as well. And the episodes are short, like <10 minutes, which makes it easy to work into the drive in to work.
The first episode I’m going to recommend is “Can hypotension from propofol be predicted?”
Propofol is a super common medication that we use for induction prior to intubation and for maintenance of sedation in the ICU. One of the big downsides of its use is the risk of hypotension. This short episode discusses ways to predict who can handle the propofol.
The second recommendation from this podcast is an episode called “Are diuretics safe to reduce fluid balance in critically ill patients?”
We use diuretics in the ICU commonly in the process of “de-resuscitation,” getting rid of all that excess fluid patients have on board thanks to our resuscitation. This podcast talks about the safety and efficacy of diuretics for this purpose.
Atrial Fibrillation
A-fib is a common problem in the ICU. Josh Farkas from the Internet Book of Critical Care does a nice discussion on the subject.
